

What would you be thinking in this case study?
Here’s a case that came into the clinic. I thought it would be interesting, because thinking globally was key in helping figure out solutions to get this runner smiling again.
I’ll break it down into the hard facts, share the things that I’ve performed, lay out the outcomes, give possible diagnoses, and offer insight as to what my thought process was when diagnosing the condition. Ready to go? Let’s do it!
HISTORY - Here’s the facts:
Sport: Distance Runner
Right side dominant 38 YO female with left medial ankle “bruising” pain traveling down into the medial arch of foot
Symptoms have been progressive for the past 7 months
Swelling noted initially; however, more intermittent with less intensity now

It felt better with resting, icing, bracing, and taping
It felt worse during the first 1/2 mile of running, pushing off, or landing
Rated it a 7-8 out of 10 (numerical rating scale)

FINDINGS - Here are the outcomes:
Vitals
Within normal limits (WNL)
Neurovascular assessment
WNL
Inspection
Patient standing - pes planus, tibial internal rotation, femoral internal rotation, popliteal crease oblique angle
L rib flare/lateral shift
Palpatory findings
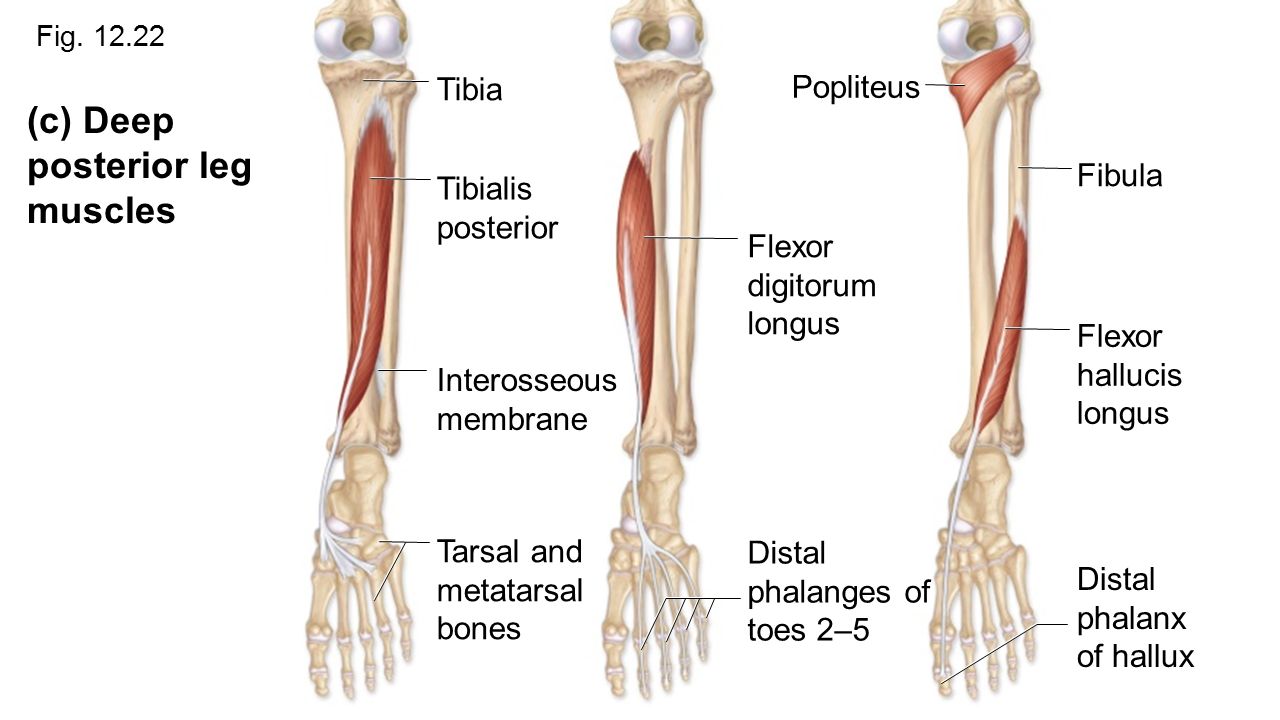
Tenderness to palpation (TTP) along the posterior tibialis, flexor hallicus longus, and flexor digitorum tendons along the inferior aspect of the medial malleolus.
TTP along the peroneals, soleus, and gastrocnemius, anterior tibiailis
Slight TTP along the medial tibial shaft
Tonicity along the hamstrings, quadriceps, adductors, gracilis, popliteus
Range of motion
Great toe - limited great toe MTP dorsiflexion compared to contralateral side
Ankle - limited ipsilateral talocrural inversion/eversion
Knee - limited tibiofemoral IR
Hip - limited ipsilateral femoroacetabular IR
Lumbar spine - limited RR
Gait assessment
R foot external rotated (heel strike - mid stance - toe off)
R hip lateral shift (heel strike - mid stance)
L foot external rotated (heel strike - mid stance - toe off)
L tibial internal rotation (heel strike - mid stance - toe off)
L femoral adduction + internal rotation (NWB stance)
L hip drop (NWB stance)
Orthopedic evaluation
(-) - Hip impingement tests
(-) - Ankle ligamentous tests
(-) - Knee ligamentous tests
(-) - Thessaly’s test
(-) - McMurray’s test
(-) - Dial’s sign
(+) March’s test - lack of movement at L SI joint, R hip hike
Other
Left anterior inferior chain (adopted from Postural Restoration Institute)
Manual Muscle Test (MMT) to check for tibiofemoral subluxation
-5/5 L>R gluteus medius/maximus, popliteus
DIFFERENTIAL DIAGNOSES - Here’s possible thoughts:
Here’s what previous clinicians diagnosed
Posterior tibialis tendinitis
Medial Tibial Stress Syndrome
Although the individual was presenting with primary complaints in the medial ankle, my job was not to only look outside the box, but rather, beyond the box. With that in mind, here’s what I was thinking:
SIJ pathology
Secondary tendinopathy (medial ankle soft tissue including posterior tibialis, FHL, FDL)
DEDUCTIVE REASONING - Here’s how I narrowed it down:
Posterior Tibialis/FHL/FDL Tendinopathology -

Inspection:
Pes planus, tibial internal rotation
Palpation:
TTP posterior tibialis tendon, FDL tendon, FHL tendon
Slight TTP along the medial tibial shaft
Talonavicular and navioculocuboid joint restrictions
Assessed end range of motion
(+) finding - limited great toe MTP dorsiflexion
MMT:
-5/5 posterior tibialis, FHL, FDL
Other:
Repetitive heel lift - discomfort noted along the medial aspect of the foot (chief complaint)
VERDICT - LIKELY
Sacroiliac Joint Pathology -
Inspection:
R anterior rotated pelvis
Palpation:
R anterior inferior PSIS
TTP B gluteals, B SIJs
MMT:
-5/5 L>R gluteus medius/maximus
Orthopedic tests:
(+) March’s Test - R hip hike with R hip flexion
(+) FABERs Test - slight discomfort in R SIJ
VERDICT - LIKELY


Medial Tibial Stress Syndrome -
Inspection:
Pes planus, tibial internal rotation
Palpation:
TTP posterior tibialis tendon, FDL tendon, FHL tendon distally (“diffuse soft tissue tenderness”)
Slight TTP along the medial tibial shaft
MMT:
-5/5 posterior tibialis, FHL, FDL
VERDICT - POSSIBLE
Yes all of these conditions are possible and likely; however, there has to be a reason for this string of issues. It is fairly obvious to recognize that this individual had complications within the ankle/foot, but the mystery of it all was why. If I couldn’t figure out the “why,” then I would be able to help her truly resolve this nagging issue.
Since other clinicians focused on the symptomatic target tissue (medial ankle) and suggested general hip stability exercises, I knew I needed to dive a little more and investigate other possible culprits.
My go-to was first to make sure the architecture was sound (my fancy way of figuring out if the surrounding joints were moving well enough to allow the demands of her sport). This meant that I had to assess the lower back, pelvis, femoroacetabular joints, tibiofemoral joints, proximal tibiofibular joints, talocrural joints, subtalar joints, and all of the other foot joints. (Yeah that’s a butt load of joints to assess). This was when I noticed that the R SIJ/public symphysis was restricted, the great toe MTP joint was not moving as well, and subtalar joints had less options for movement.
After noting that, I had to make sure the soft tissues had the needed elasticity to meet the demands of running. This is where I was able to identify numerous soft tissue sites that were bound together causing local sites of densification (aka. knots in patient/athlete lingo)
Lastly I needed to assess the possible weak links - those tissues that are either overactive or under active. I typically try to identify those under active contractile tissues, which will help narrow in on those over active tissues via reciprocal inhibition. Through it all, as I charted the problematic landscape, it also helped paint a pathway for treatment options, and provided a roadmap for correcting the issues.
So guess what happened after treatment?
Well after treating the patient with the use of soft tissue maneuvers (ie. Active Release Technique), adjustments (SIJ, foot, and ankle), and adding tissue activation methods (particularly contralateral pelvis stability exercises), the patient was able to progressively run longer and harder, and established more global ROM, all while feeling minimal to no medial ankle discomfort.
What seemed to be an ankle pathology was actually the pelvis screaming for help. Since the pelvis was faulty, she wasn’t unable to decelerate efficiently and effectively, as those pelvic musculature are a driving force that controls this movement. As a result, the smaller, less equipped muscles in the ankle had the added job of decelerating her whole body as she ran. This was what I feel caused the medial ankle symptoms that she experienced.
Here’s the take home message:
As you can see, it took a global outlook to generate a treatment pathway to correct a local issue. Through your journey in this profession, make it an effort to broaden your perspective and have an opened mind. If treating one area doesn't give the outcomes you want, then look elsewhere. Being myopic will not only limit your capabilities, but it will eventually lead to subpar results for those that you serve. You’re in this profession to change lives… and you can’t change lives if you can’t make a difference in the way they feel and move.
Thanks for being curious and taking the time to read this! Hope it added value to your life and equips you to become better than you were yesterday!

Dr. Joe Jaime, DC, DACBSP®, ATC, CSCS®, FRC®ms, CES
BONUS: I try to reflect on the cases that come through, to see how I can improve my evaluation and treatment game, so here’s some of my afterthoughts …
Here’s what I think I should’ve done to be more thorough:
Inspect shoe wear
Assess running
Navicular Drop test
Implement different and more sport-specific running exercises (I feel like I would have liked to have given more variety of movement activation options)
{kind=link}